New coronavirus variant identified in France | Science | In-depth reporting on science and technology | DW | 04.01.2022
B.1.640.2 was discovered in a traveler returning from Cameroon and has a high number of mutations. And a first "flurona" case has been confirmed in Israel.
Just when we thought things were looking up at least a little, because the omicron variant, while being more contagious, often takes a milder course than delta, a new variant has emerged. We do not yet know how dangerous it is, or even where it originated.
The new variant was detected in early December in a traveler who returned to France from Cameroon, the hospital IHU Mediterrannee in Marseille announced. The returnee from Cameroon reportedly infected 12 people in southern France.
Large number of mutations
This new mutant, called B.1.640.2, has 46 mutations in an "atypical combination," according to a preprint study that has not yet been peer-reviewed.
According to this study, the two already known spike protein mutations N501Y and E484K are also found in the new coronavirus variant. The N501Y mutation, for example, was detected very early in the alpha variant. It causes the pathogen to bind more strongly to human cells and thus to spread more easily in the body.
E484K is one of the escape mutations located directly in the spike protein and thus possibly reduces the effectiveness of COVID-19 vaccines.
Little known about danger and origin
But what these mutations mean and whether the new coronavirus variant B.1.640.2 is actually more contagious than the original SARS-CoV-2 virus cannot yet be said with any real confidence, due to the lack of available data and the small number of cases.
Jörg Timm, head of the Institute for Virology at University Hospital Düsseldorf, believes that the new variant isn't extremely dangerous.
"The variant was first described a little while ago and hasn't become more prominent in areas where a lot of sequencing is being done," he said. "It hasn't spread widely."
Timm added that this was a marked difference to the omicron variant, which researchers realized from the start would spread very quickly.
"Nobody expects that the B.1640 variant will cause truly significant problems," Timm said. "Of course you'll have to add a small question mark to that, but this is my current view of it."
We do not yet know anything about the origin of this new variant, either. The fact that B.1.640.2 has now been detected for the first time in a returnee from Cameroon does not mean that the variant has also emerged in the Central African country.
However, very low vaccination rates generally favor the emergence of new coronavirus mutations. In Cameroon, only 2.4% of the population is fully vaccinated, according to data from the Johns Hopkins University in Baltimore in the United States.
As long as the vaccination campaign isn't advanced globally, new variants will continue to develop. Sometimes they are more harmless, sometimes more dangerous. It remains to be seen how harmful this new variant will be.

Omicron attacks the lungs less severely — therefore, COVID-19 patients require artificial respiration less often
Possible reasons for milder omicron course
We already know that the omicron variant is much more contagious, and is spreading rapidly around the world. But at the same time, the courses are much milder in most patients, as ever more studies are confirming.
It is also gradually becoming clearer which factors are at work here. The T-cells of vaccinated and recovered persons react to omicron, thus protecting most infected persons from a severe course of COVID-19.
It is true that the mutations in omicron have altered the spike protein such that the antibodies generated by previous infection or vaccination are no longer as protective.
But the acquired immune response by T-cells still works in 70% to 80% of cases, similar to the older beta and delta variants, researchers from Cape Town, South Africa, found. The T-cells of vaccinated and recovered patients recognized omicron nearly as well as the original coronavirus variant, the group concluded.
Omicron attacks the lungs less severely
In addition, the omicron variant attacks the lungs much less frequently, researchers from Japan and the US found in animal studies.
Instead, the omicron variant is more likely to attack the upper respiratory tract, such as the nose, throat and trachea, according to the study, which also has not yet been peer-reviewed.
The viral load in the noses of hamsters and mice infected with omicron was just as high as with earlier mutations. But in the lungs, the viral load and thus the damage was significantly less.
In mid-December, researchers at the University of Hong Kong came to very similar conclusions. They found that although the omicron variant infects the bronchus up to 70 times faster than the delta variant and multiplies there, it spreads up to 10 times less in lung tissue.
Fewer patients need artificial respiration
These research findings are in line with observations from Great Britain. There, too, the highly contagious omicron variant is causing a sharp rise in the number of infections.
But at the same time, the statistical risk of having to be treated in a hospital is reduced by a third compared to the delta variant. The number of patients requiring artificial respiration is also largely unchanged, despite the significantly higher infection rate with omicron.
That's a reason for hope; however, concerns remain. The significantly higher case numbers are a major challenge for overburdened health care systems.
And those who have not yet been vaccinated, or recovered from a previous COVID-19 infection, can still fall seriously ill if they contract the omicron variant.
First 'flurona' case in Israel
Meanwhile, in Israel, a 31-year-old pregnant woman has contracted COVID-19 and the seasonal influenza virus at the same time. It is the world's first registered "flurona" case, a neologism composed of flu and corona.
The pregnant woman, who local paper Hamodia reported was not vaccinated against COVID-19 or the flu, was only mildly ill. Because Israel has seen a sharp increase in flu infections in recent weeks, and its Health Ministry is investigating the case to see if "flurona" could be causing more severe illness. This has stoked fears of a "twindemic" of both COVID-19 and the flu.
Israel has seen a particularly dramatic increase in severe flu cases this winter. According to the Times of Israel, nearly 2,000 people had to be hospitalized with influenza by the end of 2021.
Health authorities fear that with such a strong flu wave, there could be many more such cases of double infections coming.
This article was translated from German.
The story was adjusted on January 5 to reflect what is known about mutations in the omicron variant, also the vaccination status of the pregnant woman infected with both coronavirus and influenza. The statement by Jörg Timm was added as well.
-
COVID: SARS-CoV-2 and other viruses in pictures
Virus with a crown
May we present: The coronavirus! This is how 10-year-old Andrej from Russia views SARS-CoV-2, the virus that causes COVID-19 and is behind the pandemic that's had the world in its grip for almost two years now. The name for this virus family is derived from the Latin "corona" for crown. It was first used in 1968 and refers to the spike proteins on the virus' surface.
-
COVID: SARS-CoV-2 and other viruses in pictures
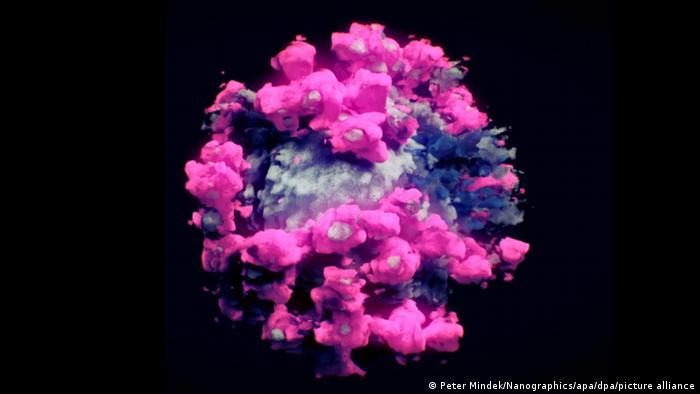
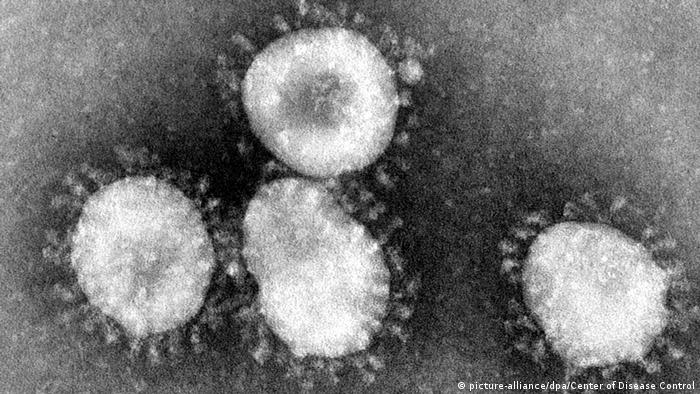
The real deal
And this is what the novel coronavirus actually looks like. Each SARS-CoV-2 particle is about 80 nanometers in diameter. Each particle contains a ball of RNA, the virus’s genetic code. That is protected by spike protein, the protusions that gave the virus its name. SARS-CoV-2 is a member of the coronavirus family, which includes the viruses responsible for SARS and MERS. More on that later.
-
COVID: SARS-CoV-2 and other viruses in pictures
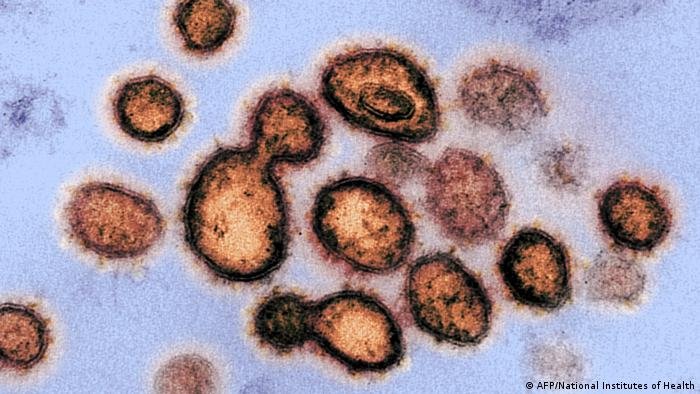
An airborne virus
SARS-CoV-2 particles are transferred through droplets and aerosols that a person emits when they breathe, cough or talk. That's why face masks have become ubiquitous during the pandemic: Health authorities recommend citizens wear them to stop the spread of the virus. It can also be transmitted via contaminated surfaces.
-
COVID: SARS-CoV-2 and other viruses in pictures
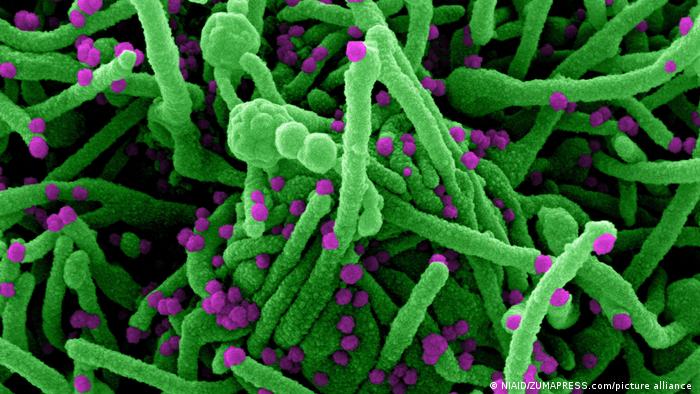
Entering human cells
SARS-CoV-2 uses its spike proteins to bind with a protein on the surface of cells. That sets off chemical changes, which allow the virus’s RNA to enter the cell (green in this image). The virus then forces the cell to make copies of its RNA. A single cell can produce tens of thousands of new virus particles (purple in this image) like this, which then infect other healthy cells.
-
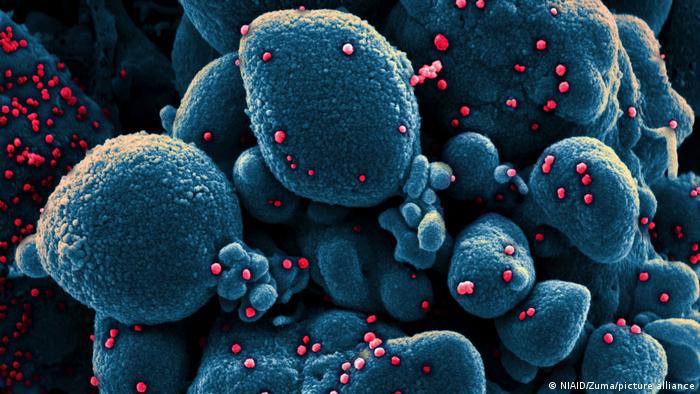
COVID: SARS-CoV-2 and other viruses in pictures
New to humans
Another electron microscope image of a cell (blue) heavily infected with SARS-CoV-2 particles (red). The virus behind our current pandemic isn't too different from viruses like the ones causing the flu or common cold. But before 2019, human immune systems hadn't seen this particular strain before, which is why no one had built up immunity.
-
COVID: SARS-CoV-2 and other viruses in pictures
SARS-CoV: The first coronavirus outbreak of the 21st century
The first time this century that humanity came in contact with a coronavirus was in China in 2002. In March 2003, the WHO issued a global alert warning of atypical pneumonia spreading quickly. SARS, or severe accute respiratory syndrome, spread to roughly 30 countries, but not all of these recorded deaths. The WHO declared the epidemic contained in July 2003.
-
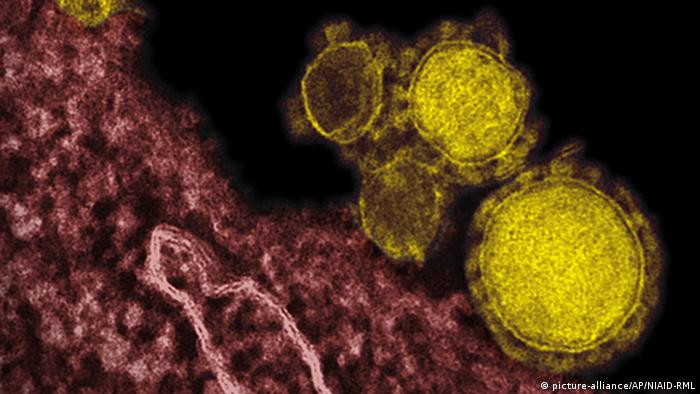
COVID: SARS-CoV-2 and other viruses in pictures
MERS-CoV, another coronavirus family member
In 2012, researchers discovered MERS-CoV, a novel coronavirus, after genome sequencing of samples from people who had fallen ill with a new flu-like illness. This illness came to be known as MERS, or Middle East respiratory syndrome, after where the first outbreak occurred. It is less infectious than COVID-19. Transmission usually occurs among family members or in healthcare settings.
-
COVID: SARS-CoV-2 and other viruses in pictures
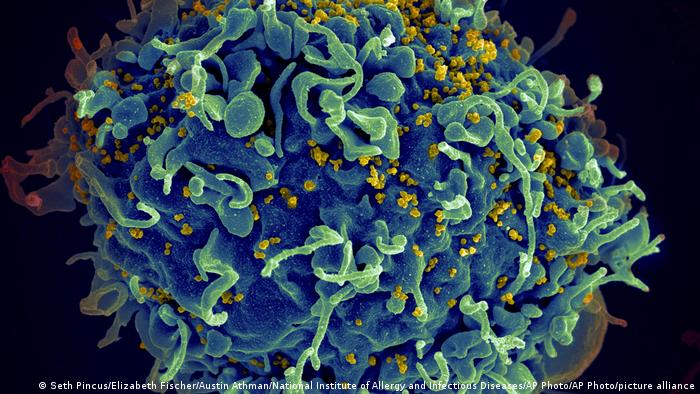
HIV: The other pandemic
The HI-virus (here in yellow), attacks the immune system, for examples T-cells (here in blue). Like SARS-CoV-2, it's an RNA-based virus. If left untreated, it'll weaken the immune system until it can't fight infections anymore. HIV is transmitted through bodily fluids like semen or blood. There's no vaccine, but there's medication that brings down the viral load and stops AIDS from breaking out.
Author: Carla Bleiker